Learn the key signs of a failing dental implant, including pain, mobility, bone loss, and infection, so you know when it’s time to intervene or remove it.
How to know when it's time to pull the plug on a failing implant.
Imagine you’re walking down the hall of your clinic, coffee in hand, feeling like the apex predator of dentistry. You just placed a beautiful implant three months ago. The tissue looked pristine. The torque was solid. You’re ready to unroof this thing, scan it, and collect your easy production.
You unscrew the healing abutment, and the patient flinches.
Your stomach drops. You stand there, not knowing how to break the silence—and utterly terrified of what that flinch means.
I see how it can be stressful. Implants are pitched to us as these infallible titanium miracles. We’re told they have a 95% success rate, which is great until you’re staring down the barrel of that 5%. When an implant fails, it feels like a personal indictment of your surgical skills. But here’s the glitch in the matrix: biology doesn't care about your ego. Sometimes, despite perfect execution, implants fail.
The difference between a good surgeon and a great one isn't a zero percent failure rate. It's the ability to recognize failure early, own it, and pivot.
Let’s clean it up. Here are the five undeniable signs that your implant is tanking.
1. The Sound of Silence (and Pain)
When someone says an implant is "integrated," they’re talking about a biological lock between titanium and bone.
How do you test that lock? You tap it. Tapping the healing abutment with the back of a mirror is the cheapest, most effective diagnostic tool in your arsenal. A healthy, integrated implant produces a hard, hollow, metallic ring. It sounds like success.
A failing implant? It produces a quiet, dull "thud." It sounds like a wet log hitting the mud. If the implant moves when tapped and doesn't make that hollow sound, it has failed to integrate.
The chaser here is pain. Normal surgical recovery pain typically lasts three to five days. If a patient experiences pain weeks or months later, it’s an early sign of failure. Furthermore, if the patient feels sensitivity or pain when you unscrew the healing abutment, you have a problem. Bone doesn't have nerve endings that register that kind of pain; soft tissue and infection do.
2. The Tremors
This is the part that really matters clinically.
Any movement of the implant when you are working on it—such as placing an impression coping or a scan body—indicates a lack of proper integration.
We aren't talking several millimeters of sway here. Even a microscopic, barely perceptible amount of mobility means the implant is dead in the water. There is no "wait and see" with a mobile implant. There is no "maybe it will tighten up." It won't. It needs to be removed.
3. The X-Ray Reckoning
X-rays are the receipts of implant dentistry. They don't lie.
When you take a PA, you are looking for two specific harbingers of doom. The first is radiolucency at the apex. A dark halo around the tip of the implant indicates an active infection. This isn't a "monitor it" situation; it requires immediate intervention, often antibiotics and eventual removal.
The second is "saucerization," or progressive bone loss around the crest or platform of the implant. A little remodeling is normal. A crater is not. While a general rule of thumb is to remove an implant with 50% or more bone loss, this decision varies by patient. But make no mistake: progressive bone loss is the market correcting your surgical hubris.
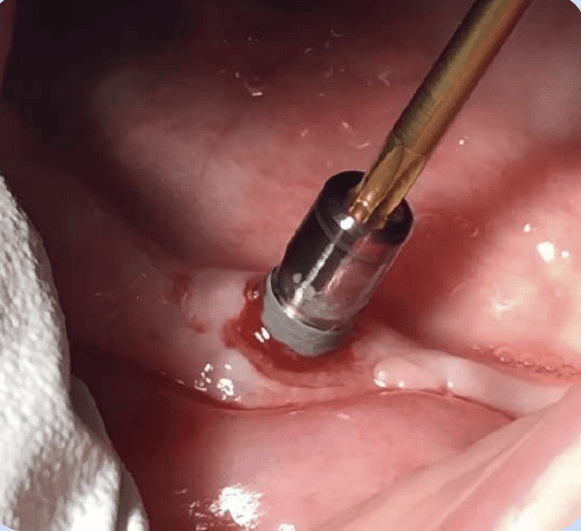
4. The Tissue Tells All
The soft tissue around a successful implant should look pink, beautiful, and pristine when the healing abutment is removed. It should look like it belongs in a textbook.
Conversely, tissue around a failing implant looks angry. It may appear red, inflamed, bleed easily when touched, or—in the worst cases—exude pus. This type of unhealthy tissue is often seen in patients with compromised healing, such as those with uncontrolled diabetes or those on long-term steroids.
The tissue is the canary in the coal mine. Ignore it at your peril.
5. The Torque Test
Finally, torque provides the definitive, undeniable test of integration.
When you are torquing a restoration onto the implant—taking it up to 35 Ncm—the patient should feel absolutely nothing. No pressure, no pinching, no pain.
If the patient feels pain during this process, it indicates the implant is not properly integrated and has likely failed, even if it feels mechanically tight to your hand. The bone hasn't locked in; fibrous tissue has. And fibrous tissue cannot support a crown.
The Bottom Line
Complications are a tax on doing business in the oral cavity. They are more common in patients with risk factors like diabetes, long-term steroid use, smoking, or periodontal disease.
But here is the brutal truth: even completely healthy patients can experience random implant failures.
If an implant hasn't integrated, the general procedure is simple, albeit frustrating. You remove it, thoroughly debride the site, perform a bone graft, and place a new implant later. The good news? The second attempt often has an excellent chance of success.
Don't let a failure paralyze you. Diagnose it, address it, and move forward.
Keep it simple, surgeon.
Ivan

